 Cell Technology Co., Ltd.")

News
News Center
All about stem cell therapy for AIDS
2021-12-01
Recently, a female internet user posted online, claiming that while shopping with her husband at a Guangzhou mall, she accidentally brushed against a man walking in the opposite direction—and immediately felt a sharp pain on the back of her hand. Shortly afterward, another male internet user shared a similar experience: while strolling through the same mall, he suddenly noticed a tiny pricking sensation on his arm, which turned out to be a minuscule needle mark accompanied by faint traces of blood. Both affected users have since expressed concern that they might have been exposed to HIV, sparking widespread panic among online communities.
Although it turned out to be a false alarm, many people still react with fear whenever AIDS is mentioned, going out of their way to avoid it altogether. After all, once infected with HIV/AIDS, there’s no cure—period.
To date, the HIV virus remains one of the world's biggest public health challenges. According to the "2020 Global AIDS Progress Report" released by UNAIDS, in 2019, the global number of people living with HIV exceeded 38 million, including 1.7 million new infections and 690,000 deaths from AIDS-related illnesses. Currently, 12.6 million people still lack access to life-saving treatment. [1] According to the "2019 National Overview of Notifiable Infectious Diseases" released by China's National Health Commission, nearly 21,000 people nationwide died from AIDS in 2019, making it the leading cause of reported deaths. [2] 。
AIDS, a disease that makes people turn pale at the mention of it
AIDS, which stands for "Acquired Immune Deficiency Syndrome," is a severe immune-system disorder caused by the HIV virus.
Once the HIV virus enters the body, it specifically targets and attacks the most critical CD4 T lymphocytes in the immune system, leaving the body defenseless against infections. If we compare the human body to a computer, AIDS would be like a virus that deliberately targets and disables the antivirus software—once the antivirus is "taken down," other harmful viruses can easily slip in and wreak havoc on the computer at will.
In this context, even a common cold or cough could potentially develop into pneumonia, tuberculosis, and ultimately claim a life. In other words, AIDS itself isn’t inherently fatal—but it serves as the "perfect accomplice" for other diseases.
Even more alarming is that, while patients may experience some acute symptoms shortly after first contracting HIV, the virus can then lie dormant in their bodies for up to over a decade. This means that, for years after infection, patients might not notice any discomfort at all. But suddenly, one day out of nowhere, they could start experiencing frequent colds, fevers, chest pain, diarrhea, and even skin ulcers—symptoms that often signal the onset of severe complications. Ultimately, what typically awaits these patients are various aggressive forms of cancer, which is why AIDS is also referred to as the "super cancer."
Current Status of HIV Treatment
Since the emergence of AIDS, developing an effective HIV vaccine has been one of science's relentless pursuits—but progress has consistently remained slow. To date, we still don’t have a commercially available HIV vaccine.
In 1991, Chinese-American scientist David Ho invented "cocktail therapy" (Highly Active Antiretroviral Therapy). This innovative approach combines several antiviral drugs to combat the HIV virus, effectively preventing the virus from developing resistance to any single medication. However, while these antiviral drugs can significantly suppress HIV replication and halt the progression of the disease, they do not completely eliminate the virus—it merely keeps it under control, allowing patients to maintain a stable condition. [3] 。
While antiretroviral therapy (ART) has proven effective in suppressing the onset of AIDS, concerns remain regarding the drugs' own toxic side effects, the growing issue of drug resistance, and the financial challenges associated with scaling up treatment early on. In addition to continuously refining treatment regimens, it’s crucial to maximize therapeutic efficacy while minimizing adverse effects. Only by achieving both the cure and prevention of HIV can we truly curb the spread of AIDS. [3] 。
In recent years, mesenchymal stem cells have been gaining widespread attention as a promising new approach for treating intractable diseases, offering fresh hope for the treatment of AIDS as well.
Stem cells hold the potential to aid in the treatment of AIDS.
Recently, a research team from the University of California, Davis, published a study titled "Gut Germinal Center Regeneration and Enhanced Antiviral Immunity by Mesenchymal Stem/Stromal Cells in SIV Infection" in JCI Insight. [4] 。
In this groundbreaking study, researchers discovered that mesenchymal stem cells can reduce HIV viral loads, boost immune function, and restore intestinal lymphoid follicles damaged by simian immunodeficiency virus (SIV, the monkey equivalent of human HIV), providing a scientific foundation for a multifaceted strategy to eradicate the AIDS virus.
The progression of HIV disease is characterized by the loss of CD4+ T cells, chronic immune activation, and immune dysfunction. While antiretroviral therapy (ART) is highly effective in suppressing HIV replication and significantly reducing morbidity and mortality, it cannot eliminate the latent HIV reservoirs within the host, nor can it directly restore immune function or repair damaged lymphoid tissues. Therefore, novel approaches are urgently needed to boost host immunity, paving the way for targeted viral eradication and complete immune recovery.
Based on a comprehensive analysis of immunology and virology, the research team found that mesenchymal stem cell therapy restored mucosal lymphoid follicle structures and boosted antiviral immunity.
Data show that systemic MSC infusion normalized CD4+ T-cell counts and the CD4+/CD8+ ratio, while also inducing significant viral reductions—both in terms of decreased plasma viral load and clearance of virus-positive cells from intestinal effector sites.
Additionally, following MSC infusion, the germinal centers (GCs) exhibited robust regeneration (Figure 1). Notably, follicular dendritic cells within the GCs demonstrated enhanced viral capture—meaning they were able to retain viruses on their cell surfaces—supporting efficient antigen presentation and promoting interactions between T cells and B cells, which in turn further amplifies antibody production.
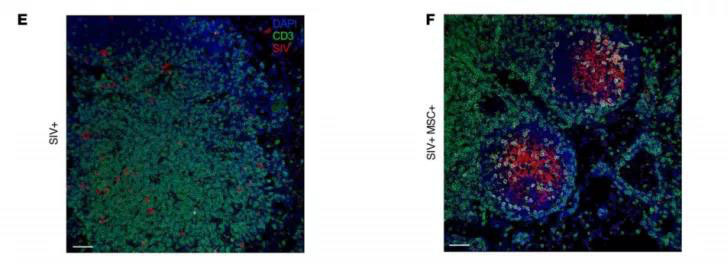
Figure 1: GC Regeneration in the SIV+MSC+ Group: Dual in situ RNA hybridization and IHC analysis of MSLN in SIV+ and SIV+, revealing viral RNA (red) and T cells (green).
HIV-infected patients exhibit widespread metabolic abnormalities, which are often linked to inflammation, immune dysregulation, and microbial translocation. The research team hypothesized that the mesenchymal stem cell-induced enhancement of antiviral immunity and reversal of viral pathogenic effects would be reflected in changes to the host’s metabolomic profile. Metabolic analysis confirmed their hypothesis: B/T helper cell activation, along with increased expression of anti-SIV antibodies and IL-7, was closely associated with robust retinol metabolism, a process that supports the gut-homing of antigen-activated lymphocytes (Figure 2).

Figure 2: Retinol Metabolism – Significant correlations were observed between retinoic acid (RA) levels, SIV-specific antibody titers, activated memory B cells, colonic CD8(227) T-cell proliferation, H-subgroup populations in peripheral blood and tissues, as well as IL-7 and GZMB expression.
This study demonstrates that mesenchymal stem cells aid in the recovery of lymphoid follicles, enabling them to regulate, reshape, and repair damaged mucosal tissues. Furthermore, as antiviral antibodies and T cells rapidly increase in the body following treatment, immune function is significantly enhanced.
In addition, on June 9, 2021, the team led by Academician Wang Fusheng, Director of the Infection Disease Diagnosis and Treatment & Research Center at the Fifth Medical Center of the PLA General Hospital and Director of the National Clinical Research Center for Infectious Diseases, published online in *Signal Transduction and Targeted Therapy* a research paper titled "Human Umbilical Cord Mesenchymal Stem Cell Transfusion in Immune Non-Responders with AIDS: A Multicenter Randomized Controlled Trial." [5] The study focuses on a multicenter, randomized, double-blind, placebo-controlled, dose-escalation Phase 2 clinical trial evaluating human umbilical cord-derived mesenchymal stem cell (hUC-MSC) infusion therapy in HIV-1 patients with immune non-responsiveness.
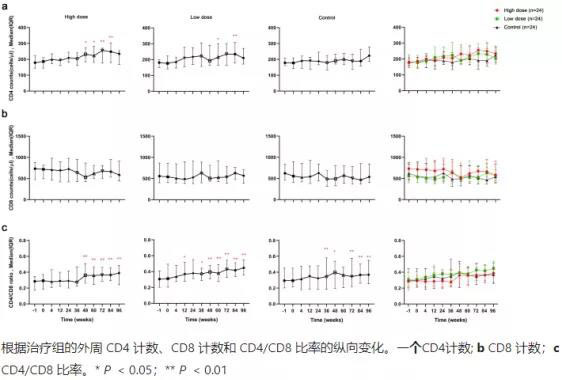
Figure 3: After 48 weeks of treatment, the hUC-MSC group showed an increase in CD4 counts. Notably, the high-dose group exhibited superior recovery of CD4 T cells compared to baseline at weeks 48, 60, 72, and 84, while the low-dose group demonstrated improved CD4 T-cell recovery relative to baseline at weeks 48, 60, and 84. In contrast, there were no statistically significant differences in CD8 counts among the high-dose, low-dose, and control groups when compared to baseline. Additionally, while the CD4/CD8 ratios within each group varied significantly, there was no notable statistical difference in the CD4/CD8 ratio among the three groups.

Figure 4: (Clinical Adverse Reactions During 96 Weeks of Follow-up) No infusion-related serious adverse events occurred in any group during the trial. Additionally, no significant differences were observed between the three groups regarding other adverse reactions, including cardiac disorders, gastrointestinal conditions, skin diseases, ENT disorders, respiratory issues, and hematological abnormalities.
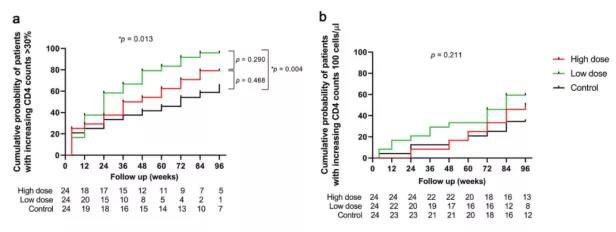
Figure 5: Based on the concept of immune responders, patients were evaluated for CD4 count increases of more than 100 cells/μL or a 30% rise compared to baseline. Results showed that the low-dose group had a significantly higher cumulative probability of patients achieving a CD4 count increase greater than 30% compared to the control group. However, there was no statistically significant difference in the cumulative probability of patients across the three groups who experienced a CD4 count increase exceeding 100 cells/μL.
The study reported that both doses of hUC-MSCs (0.5 × 10^6 and 1.5 × 10^6 cells/kg body weight) were safe and well-tolerated, with no serious transfusion-related adverse events observed (Figure 4). Additionally, the low-dose stem cell infusion proved superior to the high-dose infusion (Figure 3), and it led to at least partial improvement in patients' host immune reconstitution (Figure 5). These findings suggest a promising new therapeutic approach for HIV-1 patients who exhibit immune non-responsiveness, particularly when combined with antiretroviral therapy.
In summary, antiretroviral drugs can prevent viral infection but are unable to repair lymphoid tissues. Mesenchymal stem cells, however, have the potential to revitalize this field and restore immune function. Even in the absence of antiviral medications, mesenchymal stem cells can bolster the host’s antiviral response by repairing lymphatic follicles, reinstating mucosal immunity, and reactivating molecules that initially target viruses. Overall, mesenchymal stem cells may uncover novel roles in modulating antiviral immunity to enhance viral clearance, offering promising avenues for boosting antiviral defenses and potentially advancing combined therapeutic strategies against HIV.
The HIV virus is not an impenetrable fortress, and AIDS is by no means invincible. Moreover, the successive emergence of the "Berlin Patient" and the "London Patient" has brought new hope to AIDS sufferers, while also providing valuable experience and guidance for future clinical treatments targeting the disease. [6-7] 。
In recent years, clinical studies on using mesenchymal stem cells to treat AIDS have been steadily advancing, and the number of research findings being published is also growing. We believe that in the future, more AIDS patients will benefit from this innovative approach.
References:
[1] https://www.unaids.org/sites/default/files/media_asset/2021-global-aids-update_en.pdf
[2] http://www.nhc.gov.cn/jkj/s3578/202004/b1519e1bc1a944fc8ec176db600f68d1.shtml
[3] Jia Xiaofang, Tan Zhimi, Zhang Lijun. Advances in Research on Drug Side Effects of Cocktail Therapy for AIDS Treatment [J]. Chinese Journal of Biological Products, 32(08):929-933.
[4] Mariana G. Weber et al. Gut Germinal Center Regeneration and Enhanced Antiviral Immunity by Mesenchymal Stem/Stromal Cells in SIV Infection. JCI Insight, 2021, doi:10.1172/jci.insight.149033.
[5] Wang L, Zhang Z, R Xu, et al. Human umbilical cord mesenchymal stem cell transplantation in immune non-responders with AIDS: a multicenter randomized controlled trial[J]. Signal Transduction and Targeted Therapy, 6(1):217.
[6] Gero Hütter, M.D., Daniel Nowak, M.D., Maximilian Mossner, B.S., et al. Long-Term Control of HIV by CCR5 Delta32/Delta32 Stem-Cell Transplantation. N Engl J Med 2009; 360:692-698
[7] Ravindra K. Gupta, Sultan Abdul-Jawad, Laura E. McCoy, Hoi Ping Mok. HIV-1 remission following CCR5Δ32/Δ32 hematopoietic stem-cell transplantation. Nature volume 568, pages 244–248 (2019)
Previous:
Related News

Here is the title—h1 placeholder text


Copyright © Jiuzhitang Maker (Beijing) Cell Technology Co., Ltd.
Powered by: 300.cn SEO | Privacy Policy