 Cell Technology Co., Ltd.")

News
News Center
Understand in One Article: The Mechanism Behind Mesenchymal Stem Cell Therapy for COPD
2021-06-21
Life depends on a single breath—but once you develop COPD, taking a deep, effortless inhale becomes harder than reaching for the stars. Imagine being buried alive, with dirt already pressing against your throat; or picture yourself climbing a mountain, only to feel as though something—a lump of blood, perhaps—has lodged painfully in your windpipe. These are the very real experiences of people living with chronic obstructive pulmonary disease.
Chronic Obstructive Pulmonary Disease (COPD), short for "Chronic Obstructive Lung Disease," is a common and widespread respiratory condition characterized by high prevalence and mortality rates. Its main symptoms include chronic cough, sputum production, shortness of breath or difficulty breathing, and chest tightness.
According to data from the World Health Organization, there are approximately 210 million COPD patients worldwide, with more than 3 million deaths annually. In China, if smoking and air pollution remain uncontrolled, the number of COPD patients could soar to over 3 million by 2030. [1] Additionally, as China's population ages, it is projected that by 2050, the number of Chinese residents aged 60 and older will reach 498 million. [2] As age increases, the incidence of pulmonary fibrosis and chronic obstructive pulmonary disease (COPD) also gradually rises—and these diseases are closely linked to aging. In fact, certain tissue structural and molecular phenotypic changes that occur during the aging process may play a key role in driving this progression. [3] 。
Cellular Senescence Mechanisms in COPD Patients
According to previous research, cellular senescence can contribute to chronic obstructive pulmonary disease through at least two non-exclusive mechanisms. First, in COPD, there is an increased rate of apoptosis in epithelial and endothelial cells, leading to the loss of cells within the alveolar walls. Under these circumstances, compensatory mechanisms involving cell proliferation should ideally be activated to counteract the depletion of alveolar cells. [4] When cellular senescence occurs, cells lose their ability to proliferate, and the balance shifts toward apoptosis, ultimately contributing to the development of chronic obstructive pulmonary disease. Additionally, evidence suggests a strong link between cellular senescence and inflammation: senescent cells can activate NF-κB and release a variety of pro-inflammatory cytokines, leading to heightened inflammatory responses. [5] 。
These aging-related pro-inflammatory mechanisms have been confirmed in human lung tissue—for instance, studies have shown that TNF-α expression levels were significantly elevated in p16-positive type II alveolar epithelial cells compared to the control group. Moreover, the degree of senescence in these p16-positive cells was positively correlated with the severity of inflammation in chronic obstructive pulmonary disease. [6] 。
Additionally, cellular senescence has been shown to be closely linked to the development of idiopathic pulmonary fibrosis. Hecker et al. [7] It was discovered that the lungs of aged mouse models with pulmonary fibrosis contain an abnormal number of senescent and anti-apoptotic myofibroblasts, and these cells were also shown to play a critical role in the progression of ongoing lung fibrosis (see Figure 1). Additionally, research indicates that bronchial epithelial cell senescence is a key factor in the pathogenesis of idiopathic pulmonary fibrosis, closely linked to the process of epithelial regeneration in patients' airways—and this regenerative capacity can be inhibited by SIRT6 antagonism. [8] 。
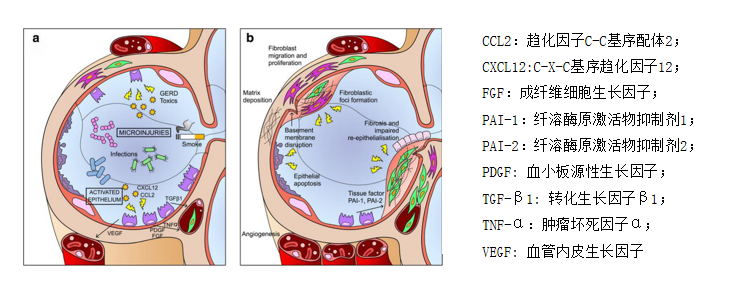
Figure 1: Schematic diagram of the pathogenesis of IPF. Repeated injury over time leads to maladaptive repair processes, characterized by AEC2 apoptosis, proliferation, and epithelial-mesenchymal crosstalk (a), followed by fibroblast and myofibroblast proliferation and excessive accumulation of extracellular matrix (b).
Aging is also accompanied by the aging and depletion of stem cells, a phenomenon that significantly hampers tissue and organ repair. As a result, the lungs of aged animals become more susceptible to fibrosis when exposed to both internal and external stimuli. [9] 。
The Treatment Bottleneck in COPD
Currently, treatments for pulmonary fibrosis and chronic obstructive pulmonary disease (COPD) primarily include non-pharmacological management options—such as pulmonary rehabilitation, supplemental oxygen therapy, and surgical interventions—as well as pharmacological approaches like corticosteroids, immunosuppressants, bronchodilators, and targeted therapies. However, these treatment strategies come with significant limitations: For instance, in non-pharmacological care, patients often struggle to adhere to prescribed pulmonary rehabilitation programs; meanwhile, the availability of lung transplants and the risk of rejection remain major challenges. On the pharmacological front, corticosteroids and immunosuppressants can lead to numerous side effects and fail to reverse existing tissue damage. Additionally, while bronchodilators have not been proven to significantly improve survival rates, targeted therapies are currently limited in their effectiveness. [10-11] 。
Extensive theoretical and practical research has confirmed that stem cells are driving advancements in regenerative medicine, playing an immeasurable role in combating serious diseases and potentially revolutionizing traditional medical approaches such as drug and surgical treatments. At the same time, they are also paving the way for innovative therapies for patients with chronic obstructive pulmonary disease.
Mesenchymal Stem Cell Therapy for COPD
Based on current research, mesenchymal stem cells primarily exert their effects on pulmonary fibrosis and chronic obstructive pulmonary disease through five key mechanisms.
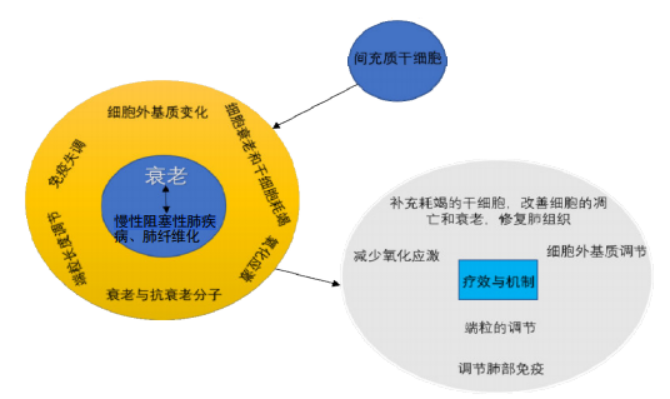
Figure 2: Effects and Mechanisms of Mesenchymal Stem Cell Transplantation in Treating Chronic Obstructive Pulmonary Disease and Pulmonary Fibrosis.
Telomere Regulation: Lung diseases are associated with telomere alterations, and research shows that patients with idiopathic pulmonary fibrosis can reduce telomere shortening—and improve their condition—through treatment with mesenchymal stem cells. [12-13] Mesenchymal stem cells may slow the progression of lung diseases and improve lung function by reducing telomere attrition in alveolar epithelial cells, fibroblasts, and other cell types.
Reducing oxidative stress: Gradually increasing oxidative stress during the aging process is a key factor contributing to lung diseases. By alleviating oxidative stress, it’s possible to improve age-related deterioration of lung tissue, reduce the incidence of lung diseases, and slow the progression of chronic lung conditions. Research has shown that mesenchymal stem cells effectively mitigate excessive oxidative stress in tissues. Reactive oxygen species are byproducts generated when cells metabolize oxygen, and they are closely linked to oxidative stress.
Liu et al. [13] It was discovered that bone marrow mesenchymal stem cells can effectively reduce reactive oxygen species in lung tissue of rats with lung injury, thereby alleviating pulmonary damage. Huang et al. [14] Research has found that implanting bone marrow mesenchymal stem cells significantly increased superoxide dismutase activity and total antioxidant capacity in the lung tissue of a mouse model with pulmonary fibrosis, suggesting that mesenchymal stem cells can alleviate oxidative stress in lung tissue. Additionally, malondialdehyde and heme oxygenase-1 are two substances with opposing effects: while the former enhances oxidative stress, the latter exerts antioxidant and cytoprotective functions. Fredenblibgh et al. [15] It was discovered that mesenchymal stem cells can reduce pulmonary malondialdehyde levels while simultaneously increasing heme oxygenase-1 synthesis.
Replenishing depleted stem cells, modulating relevant molecules, and improving cellular apoptosis and aging to repair lung tissue: Mesenchymal stem cells can serve as a supplement to already exhausted stem cells, offering anti-apoptotic effects that may help treat pulmonary fibrosis and chronic obstructive pulmonary disease. Currently, it has been reported that bone marrow-derived mesenchymal stem cells can differentiate into alveolar epithelial cells both in vivo and in vitro, and they are capable of successfully engrafting in the lungs. For instance, Huang et al. [16] It was found that intravenous implantation of bone marrow mesenchymal stem cells can reduce the severity of pulmonary fibrosis in rats and enable these cells to engraft in the lungs of the animal model, where they differentiate into type II alveolar epithelial cells. Liu et al. [17] It was found that human umbilical cord mesenchymal stem cells transplanted into a mouse model of lung injury effectively suppress cellular senescence and apoptosis, with mesenchymal stem cells successfully engrafting in the lung tissue. Additionally, these mesenchymal stem cells can secrete various factors at specific sites to inhibit tissue degeneration and promote lung repair, as shown in Figure 3.
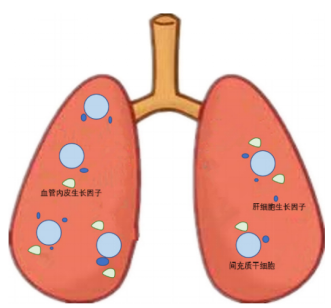
Figure 3: Mesenchymal stem cells secrete cytokines in the lungs. These cells release hepatocyte growth factor and vascular endothelial growth factor in the lung, promoting the repair of pulmonary damage.
Regulating pulmonary immunity: Lung diseases are closely linked to diminished systemic immunity and immune dysregulation. The low immunogenicity and immunomodulatory properties of mesenchymal stem cells have been widely recognized. [18] Gupta et al. [19] Proof shows that mesenchymal stem cell transplantation reduces the levels of the pro-inflammatory cytokine TNF-α in bronchoalveolar lavage fluid of mice with chronic obstructive pulmonary disease, while simultaneously increasing the anti-inflammatory cytokine IL-10. Additionally, it effectively ameliorates lung injury induced by endotoxin. Similarly, Li et al. [20] It was also reported that mesenchymal stem cells significantly suppress lung inflammation in mice with pulmonary fibrosis and can even improve the extent of fibrosis. Jackson et al. [21] Researchers have discovered that mesenchymal stem cells can transfer their own mitochondria into macrophages via tunneling nanotube-like structures, thereby modulating macrophage function and enhancing their ability to engulf bacteria, as shown in Figure 4.
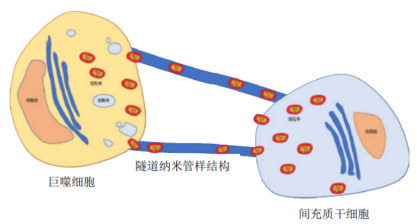
Figure 4: Mesenchymal stem cells transfer mitochondria to macrophages via tunneling nanotube-like structures.
Regulating the extracellular matrix: In lung diseases, the extracellular matrix undergoes significant alterations. Several studies have now demonstrated that mesenchymal stem cells can act as regulatory agents, helping to reverse the pathological changes in the extracellular matrix. Moodley et al. [22] In mice that developed pulmonary fibrosis due to bleomycin, collagen deposition can be modulated by mesenchymal stem cells. Meanwhile, Fikry and colleagues [23] Evidence was found of reduced collagen deposition in a rat model of pulmonary fibrosis treated with mesenchymal stem cells. Additionally, mesenchymal stem cells can reverse the expression of matrix metalloproteinase-9 and matrix metalloproteinase-12 by decreasing trypsin activity, thereby modulating extracellular matrix changes in lung tissues of a chronic obstructive pulmonary disease model, alleviating emphysema lesions, and improving lung function. [24] 。
Hypoxia enhances the potency of bone marrow mesenchymal stem cells.
Mesenchymal stem cells not only possess self-renewal and differentiation capabilities but also can secrete a variety of bioactive factors—such as nerve growth factor, vascular endothelial growth factor, vascular endothelial growth factor receptor 2, and basic fibroblast growth factor—at sites of aging or injury. Additionally, they can communicate signals by interacting with other cells and even transfer their own functional structures, like mitochondria, into damaged cells. These unique properties enable mesenchymal stem cells to exert immunomodulatory effects, protect against apoptosis, promote angiogenesis, and stimulate the proliferation and differentiation of local stem/progenitor cells. As a result, mesenchymal stem cells may represent an effective therapeutic approach for age-related chronic obstructive pulmonary disease and pulmonary fibrosis. [25] 。
Jiuzhitang Maker's U.S. partner, Stemedica, has developed its clinical-grade cell production platform, BioSmart, at the company's cGMP facility in California. TM The platform simulates the microenvironment of cells within the human body, and under continuous low-oxygen conditions, it enhances the ischemia-tolerant capabilities of human bone marrow-derived mesenchymal stem cells (it-hMSCs), enabling them to play a more significant role in treating chronic obstructive pulmonary disease.
Currently, an increasing number of clinical studies are exploring the safety and efficacy of stem cell therapy for chronic obstructive pulmonary disease, and significant breakthroughs have already been made. We believe that one day, stem cell treatment for COPD will advance even further, bringing much-needed relief to patients and significantly improving their quality of life.
In the future, Jiuzhitang Maker will continue to intensify its R&D efforts in the stem cell field, driving the translation and application of research findings to benefit human health.
Related News

Here is the title—h1 placeholder text


Copyright © Jiuzhitang Maker (Beijing) Cell Technology Co., Ltd.
Powered by: 300.cn SEO | Privacy Policy