 Cell Technology Co., Ltd.")

News
News Center
Does the more stem cells used, the better the treatment effect?
2021-04-28
Many people believe that the more stem cells used, the better—but is that really true? Here, we can clearly tell you that this idea is completely mistaken.
Take mesenchymal stem cells (MSCs) as an example: if we consider MSCs to be a "drug," there’s definitely a range where higher doses lead to better therapeutic effects. However, once you reach a saturation point—beyond which increasing the cell dose no longer enhances efficacy—you may even risk triggering a "cytokine storm." This dangerous immune response can cause shock and, in severe cases, lead to death.
When a large number of MSC cells flood the body, the massive cytokines they produce trigger excessive vasodilation and dramatically increase vascular permeability, leading to tissue redness and swelling, as well as organ damage. Moreover, these same cytokines, carried by the bloodstream to other organs, can provoke equally intense immune responses elsewhere. Such an uncontrolled immune reaction often results in multi-organ damage—or even organ failure—ultimately leading to shock and death. Clinically, this phenomenon is referred to as a "cytokine storm," as illustrated in Figure 1.
For example, cardiac muscle cells can be severely ravaged by an excessive influx of cytokines, leading to fulminant myocarditis or even sudden death; and if the cytokine storm occurs in the lungs, [1] , the lungs experience blood vessel dilation, tissue swelling, and a massive influx of immune cells—conditions that not only block the airways but also cause excessive mucus production, completely filling the respiratory system’s passages (literally "flooding" the entire lung). In other words, patients end up drowning in their own secreted mucus, preventing air from entering or leaving the lungs and halting the vital process of oxygen exchange in the alveoli. At this critical stage, supportive therapies such as intubation or ECMO are essential to help the body weather the "storm." However, if the patient fails to survive, the "cytokine storm" becomes an unforgiving killer.
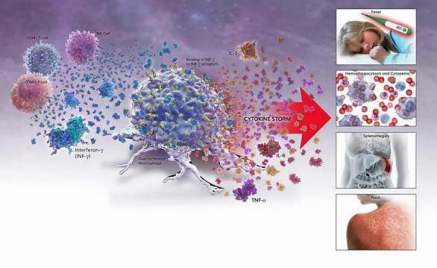
Figure 1: Cytokine Storm
In fact, there are many factors that influence the effectiveness of cell therapies—so we shouldn’t focus solely on dosage, but rather pay closer attention to cell quality and whether clinical application is being carried out correctly.
Key factors influencing MSC-related therapeutic efficacy
In preclinical studies of the therapy, animal experiments have not yet fully identified the minimum effective dose or the maximum saturating dose of MSCs. Moreover, factors such as variations in culture systems across different laboratories and differences in the source characteristics of MSCs often lead to inconsistencies in MSC quality, directly impacting the outcomes of both animal experiments and clinical trials involving MSCs. As a result, preclinical data on MSCs are insufficient to reliably guide the design of clinical study protocols. The key factors influencing MSC efficacy, in order, are: cell quality, route of administration, timing of treatment, and optimal dosage.
 Cell quality [2]
Cell quality [2]
There are inevitably some differences in quality among identical cell products manufactured by different companies, particularly when comparing imported versus domestically produced ones. The same issue also arises between different batches produced by the same manufacturer. In my view, cell quality refers to the biological potency associated with a given number of cells—or even a single cell—where higher potency indicates better cell quality. Importantly, we should discuss this potency within the context of a specific therapeutic indication. For instance, MSCs possess both immunosuppressive and pro-angiogenic properties, making them suitable for treating two distinct categories of diseases. Consequently, there are two separate biological potency metrics that correspond to these functions. When evaluating the quality or biological efficacy of MSCs, it’s crucial to always tie the discussion back to the particular clinical application at hand.
Some consensus parameters can reflect the quality of mesenchymal stem cells, such as cell viability, donor characteristics, clonogenic potential, cell size, immunosuppressive ability, and cytokine secretion levels. It can be said that cell quality is the most critical factor determining the success or failure of treatment.
Injection route [3]
Local injection route: Common sites for local MSC injections include the brain, limb muscles, heart, liver, and lumbar spine (subarachnoid space). When human bone marrow-derived MSCs were locally microinjected into the striatum of rat brains, their presence was still detectable after 72 days, and these MSCs were observed to migrate toward the corpus callosum and cerebral cortex. Additionally, when MSCs were injected locally into the right caudate nucleus of the brain, MSCs could be detected in multiple brain regions even four weeks later—and notably, their migration pattern within the brain appeared to follow the orientation of blood vessels.
Systemic injection route: Common sites for systemic MSC injection include the abdominal cavity, as well as intravenous and intra-arterial routes. After intraperitoneal injection of MSCs into immunodeficient mice (such as nude mice and NOD/SCID mice), these cells were detectable in multiple tissues and organs throughout the body for up to 120 days. In contrast, MSCs injected into immunocompetent, allogeneic mice persisted for just over 20 days, but could survive for more than 40 days when administered to syngeneic mice (see Figure 2). Following intravenous injection of MSCs, the majority of the cells initially accumulate in the lungs before being carried via the bloodstream to organs such as the liver, kidneys, and spleen. Notably, within one hour after injection, 50–60% of the MSCs remain trapped in the lungs; this percentage drops to about 30% after three hours and remains stable until 96 hours post-injection. Once localized in the lungs, MSCs are activated by the local microenvironment, prompting them to secrete potent anti-inflammatory factors. These cytokines are then distributed systemically via the bloodstream, helping to reduce widespread inflammation and modulate immune responses effectively.
The baboon experiment demonstrated that after peripheral intravenous injection, there was no significant difference in the distribution of autologous versus allogeneic mesenchymal stem cells (MSCs) within the body. Interestingly, MSCs from older donors tended to accumulate more readily in the lungs—this phenomenon was closely linked to the levels of integrin α4 and α6 expressed on their cell surfaces; higher expression correlated with reduced lung retention. In contrast, arterial injection allowed MSCs to reach and concentrate directly at the target lesion site, minimizing loss during circulation. However, when injected via the internal carotid artery, MSCs typically survived in the brain for no longer than two days.
Different injection routes—such as local injection, intravenous injection, and arterial injection—significantly influence the retention time of MSCs in vivo and are closely linked to the rate at which MSCs are cleared from the body.
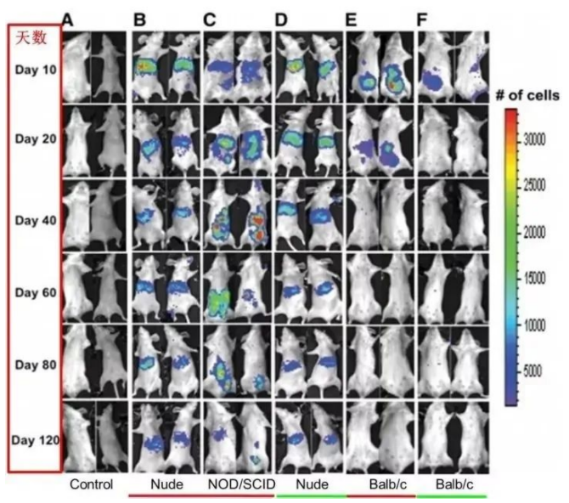
Figure 2: Distribution of MSC after intraperitoneal injection into immunodeficient mice—nude mice and NOD/SCID mice
Timing of treatment [4-6]
Pig experiments on acute liver failure revealed that a severe inflammatory environment significantly limits the effectiveness of MSCs, as these cells exhibit low survival rates in the presence of intense liver inflammation. While MSCs failed to improve survival rates in patients with acute or chronic liver failure accompanied by systemic inflammation, reducing inflammation markedly enhanced the therapeutic benefits of MSC treatment. Additionally, in a multicenter clinical study evaluating MSC therapy for children with steroid-refractory GVHD, early intervention with MSCs proved more effective than treatment initiated at later stages of the disease. These findings clearly suggest that a highly inflammatory environment may diminish the therapeutic efficacy of MSCs.
Currently, cell therapy holds three promising prospects: (1) Subclinical patients can benefit from preventive treatment when the disease is in its early stages or identified as high-risk; (2) Clinical patients may receive preventive therapy to slow disease progression; and (3) Patients in the progressive stage should undergo treatment before experiencing catastrophic organ tissue loss. Importantly, the development of any therapeutic strategy must carefully balance clinical benefits against potential side effects. To maximize the anticipated therapeutic outcomes, it is prudent to first assess the patient’s inflammatory status based on an initial risk stratification—categorized as very high-risk, high-risk, or low-risk—and then tailor the choice of MSC-based treatment approach and timing accordingly.
Optimal dosage [7]
Currently, clinical studies show significant variation in the dosage of MSCs used, with each patient receiving anywhere from just over 40,000 to more than 100 million MSC cells. In October 2020, Gaetano et al. published "Mesenchymal Stromal Cell Therapy in the Management of Perianal Fistulas in Crohn's Disease" in Medicina, summarizing trials conducted between 2013 and 2020 that focused on Crohn's disease (CD), as illustrated in Figure 3. The study revealed that the typical dose of bone marrow-derived mesenchymal stem cells used was 3 × 10^6 cells. 7 The experimental dose group achieved higher therapeutic efficacy compared to the low-dose administration group (1 × 10). 7 ) and the low-dose administration group (9 × 10 7 ); similarly, low-dose administration group (4.33 × 10<|endofcontentisolation) 7 ) showed greater efficacy than the high-dose administration group (17*10 7 )。
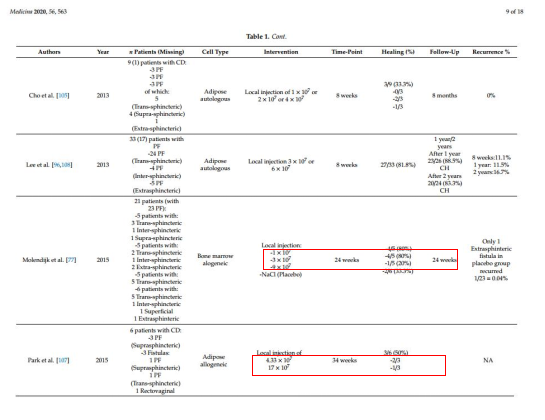
Figure 3: Trials for Crohn's Disease (CD) from 2013 to 2020
This phenomenon is far from coincidental—further research reveals that, after extraction and expansion, the optimal dose group of mesenchymal stem cells exhibited greater genetic and morphological stability, as well as enhanced proliferative capacity and angiogenic properties. [8-10] Additionally, the biggest advantage lies in the high expression of growth factors, which reduces blood compatibility issues. [11] 。 The study concluded that the optimal dose of MSC depends on the specific disease, the current severity of the condition, and the method of administration.
Currently, ensuring rational drug use—guaranteeing that medications are safe, effective, and cost-efficient for patients—has become an issue that healthcare institutions cannot afford to ignore. To prevent adverse reactions associated with MSCs, while it’s crucial for cell product manufacturers to maintain stringent quality control, proper clinical application is even more critical. Physicians must pay close attention to the issue of overuse, continuously deepen their understanding of relevant medical theories, actively engage in case discussions, and rigorously enforce applicable regulations—ultimately safeguarding the responsible and optimal clinical use of MSCs.
As the saying goes, "When illness strikes, it feels like a mountain collapsing; yet when it fades, it’s as if pulling out a thread." The clinical application of mesenchymal stem cells is just like a gentle spring rain—no thunderstorm is needed, but it must fall at precisely the right moment. Indeed, as the poem beautifully puts it: "A timely rain knows its season, silently nourishing all things."
References:
[1] 2019-novel coronavirus (2019-nCoV) infections trigger an exaggerated cytokine response that exacerbates lung injury.
[2] Analysis of Oct4-Dependent Transcriptional Networks Regulating Self-Renewal and Pluripotency in Human Embryonic Stem Cells
[3] Cell Delivery Routes for Stem Cell Therapy to the Heart: Current and Future Approaches
[4] Impact of Timing on the Efficacy and Safety of Intracoronary Autologous Bone Marrow Stem Cell Transplantation in Acute Myocardial Infarction: A Pooled Subgroup Analysis of Randomized Controlled Trials
[5] Timing and cell dose determine the therapeutic effects of bone marrow stromal cell transplantation in a rat model of cerebral infarction
[6] Into the Eye of the Cytokine Storm
[7] Mesenchymal Stromal Cell Therapy in the Management of Perianal Fistulas in Crohn's Disease: An Up-to-Date Review
[8] Kim, Y.; Kim, H.; Cho, H.; Bae, Y.; Suh, K.; Jung, J. Direct comparison of human mesenchymal stem cells derived from adipose tissue and bone marrow in mediating neovascularization in response to vascular ischemia. Cell Physiol. Biochem. 2007, 20, 867–876. [CrossRef] [PubMed]
[9] Kern, S.; Eichler, H.; Stoeve, J.; Klüter, H.; Bieback, K. Comparative analysis of mesenchymal stem cells derived from bone marrow, umbilical cord blood, or adipose tissue. Stem Cells 2006, 24, 1294–1301. [CrossRef]
[10] Izadpanah, R.; Trygg, C.; Patel, B.; Kriedt, C.; Dufour, J.; Gimble, J.M.; Bunnell, B.A. Biological properties of mesenchymal stem cells derived from bone marrow and adipose tissue. J. Cell Biochem. 2006, 99, 1285–1297. [CrossRef] [PubMed]
[11] Nikolic, M.; Stift, A.; Reinisch, W.; Vogelsang, H.; Matic, A.; Müller, C.; von Strauss und Torney, M.; Riss, S. Allogeneic expanded-adipose-derived stem cells in the treatment of rectovaginal fistulas in Crohn’s disease. Colorectal Dis. 2020. [CrossRef]
Related News

Here is the title—h1 placeholder text


Copyright © Jiuzhitang Maker (Beijing) Cell Technology Co., Ltd.
Powered by: 300.cn SEO | Privacy Policy